One rural GP surgery embraced tech to overhaul the way it engaged with patients about cardiovascular health – with dramatic results. GP partner Dr Talha Sami explains.
The growing burden of chronic disease management and Quality and Outcomes Framework (QOF) changes within primary care means practices have to be as innovative as they can when it comes to patient education and follow-up.
For instance under QOF this year, despite there being more points to be gained for the two cholesterol indicators, CHOL003 and CHOL004 some of the targets have been revised. QOF guidance for 2025/2026 sets out a target threshold of 70-95% worth 38 points for CHOL003 and a target threshold of 20-50% worth 44 points for CHOL004.
With QOF points sitting at potentially £225 each, those 82 points in 2025-2025 are worth thousands of pounds. However, successfully initiating lipid-lowering therapy often requires considerable patient engagement and persuasion. This highlights the pressing need for new and increasingly efficient strategies to target eligible patients, while also aiming to reduce reliance on face-to-face appointments.
To address these challenges, Chiddingfold Surgery, a rural dispensing practice in Surrey with a 5,174-patient list-size, has implemented a novel communication strategy for lipid-lowering therapy (LLT) management that uses digital tools to enhance clinical practice without compromising high standards of patient care.
The new virtual model has led to significant improvements in efficiency, patient engagement, and practice financial outcomes. How?
Why did we change our approach to LLT management?
Amid escalating workload pressures, adoption of alternative approaches has become essential. Previously, the practice used text messages to engage with patients about starting statins when clinically indicated.
However, the success of that was limited – it would lead to around 15% of patients accepting lipid lowering therapy and 21% of patients rejecting treatment outright. All on the basis of a simple text message.
Coincidentally, around the same time in 2023 our patient participation group (PPG) was advocating for enhanced virtual access and for the practice to make more use of digital when engaging with patients. So, in collaboration with the PPG, we moved to video production for disseminating key updates, such as our winter health and vaccination drive video, via social media.
This new pioneering approach facilitated the piloting of a cholesterol counselling video. We decided to make this part of our SMS ‘outreach’ to patients, alongside a comprehensive lipid-lowering therapy information pack. This essentially generated a virtual consultation that would replace a traditional face-to-face consultation.
What did we do differently?
Although texting patients about straightforward tasks is routinely done (such as booking for seasonal vaccines), it is much less common to use this method to trial or offer medicines for simple chronic disease management. This was a novel approach.
Previously, our simple text message-based approach read: ‘Your doctor wishes you to consider a statin. Please respond’.
Using this wording, we found that 21% of patients rejected cholesterol lowering therapy immediately.
And being a small, rural surgery, inevitably it meant that follow-ups with patients would be needed via a GP appointment, adding to workload.
Given we were aiming to move to a more digital approach (as I explained above), we developed a new clear communication aid consisting of written information and a video pack focused on lipid-lowering therapy. Trialling such a new measure, we kept costs low by:
- Partners scripting the video together to ensure clarity
- Shooting the video on one of our smart phones
- Having some prior video editing knowledge I edited it on my own laptop).
Importantly, we also changed the wording of the SMS to this, (as an example): ‘Your cholesterol reading was 6.5. It needs to be 4. Please see the attached video for more information about this figure, what it means and taking lipid lowering therapy. Tor respond click this link.’
Our workflow looked like this:
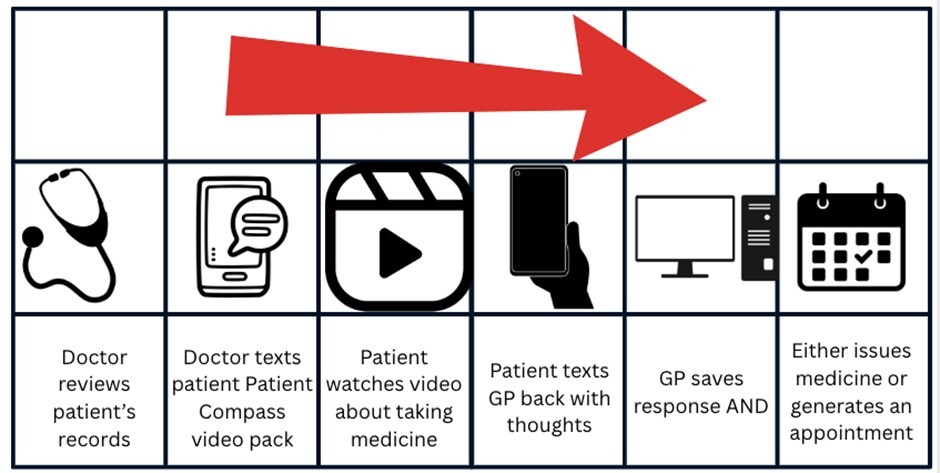
To reduce the GP workload even more, we also worked with our dispensary to target the relevant patients.
We trained dispensary staff, such as medicine checkers, so they understood the patient journey and the new virtual consultation we were using. They were then able to text the video to patients themselves or even call them up.
Overall, the new approach led to only 8% (down from 21%) of patients rejecting cholesterol lowering therapy. And personalised video messaging for cholesterol management doubled immediate lipid-lowering therapy uptake from the previous response rate of 15% to 31% of patients.
What were the benefits for the practice?
We carried out an audit of the 148 patients that needed lipid lowering therapy. It showed that over a 15 month-period, the new communication aid brought substantial benefits. These included:
Time saving – there was a 31% reduction in GP appointments among the 148-patient cohort as a result of the new measure.
Cost savings – the reduction in appointments led to a cost saving of £1880.
Profit generation – it significantly contributed towards us meeting the QOF targets for CHOL003 (14 points) and CHOL004 (16 points) and bringing in income of £6,390.
Patient and clinician feedback – there was positive feedback from both patients and clinicians.
Sustainability – this model is environmentally-friendly due to reduced patient travel and optimised resource use.
Furthermore, the practice’s performance around cholesterol management has improved.
Data collated by Surrey Heartlands ICB from the national primary care Cardiovascular Disease Prevention Audit (CVDPREVENT), which measures national health indicators, showed that our practice ranks first out of our ICB practices in five CVD indicators.
Overall, this approach has been presented as a model to emulate at our ICB meetings and received local media coverage. It was also awarded a certificate of innovation by Surrey Heartlands Health and Care Partnership, Surrey County Council and the NHS.
What were the benefits for our patients?
- Crucially, more patients received the treatment they needed – 31% (47 patients) of the patient population group we contacted using our new model started lipid lowering therapy and fewer patients rejected lipid lowering therapy.
- Patients were saved an inconvenient trip to the surgery for a face-to-face consultation having received a virtual consultation.
- Making the process more virtual contributed to us being more environmentally friendly, with less patient travel and a move away from using printed information leaflets.
- This initiative opened a direct communication channel, enabling patients to text us back with quick confirmations or more extensive replies.
Some of the patient feedback captured included: ‘Video was very informative and useful, thank you. I will undertake more research on statins prior to considering taking them.’ And, ‘Thank you for forwarding the video link to me. It is helpful and based on my latest test results I have decided to go back onto statins’.
What were the main lessons learned?
On reflection such a process only worked due to several factors. This included a willing patient population group supported by the PPG; dynamic staff that adapted to change; confident medical staff who are camera friendly; and ongoing refinement of the patient journey that was regularly disseminated to all staff members.
Future Developments
In feedback, we noticed that patients often asked about alternatives to taking medicines. In response, we developed a healthy living video discussing lifestyle modifications too.
Dr Talha Sami is a GP partner at Chiddingfold Surgery, Surrey and also works as a media contributor.


